|
Missouri Durable Medical Power of Attorney Form |
The Missouri durable medical power of attorney is created to allow a Principal to appoint an `Agent`, a person who can act as the power of attorney with regards to the patient`s health care in case they become so ill and are unable to make such decisions themselves. This document requires attestation by two (2) witnesses and a notary public in accordance with § 404.705, § 459.015.
How to Write
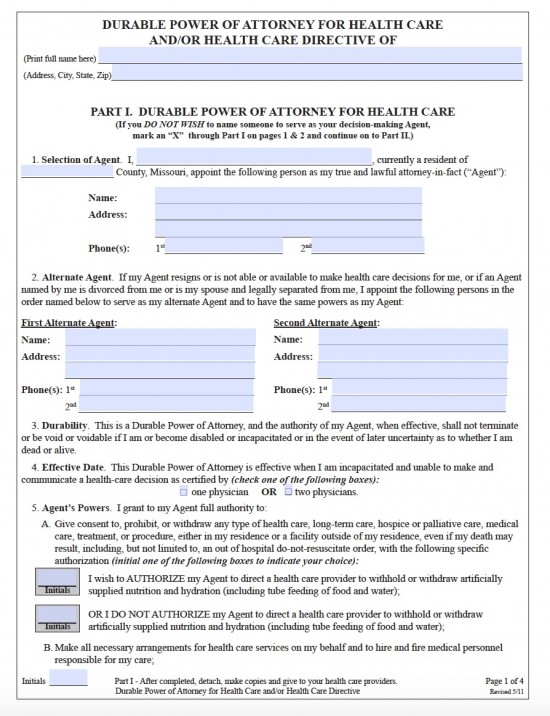
Durable Power Of Attorney For Health Care: Part 1
The principal must enter their details.
- Initial the bottom left of every page.
- Name.
- Address.
1 & 2) The agent and alternative agent must enter their details.
- Principals name.
- County of residence.
- Name of agent.
- Address.
- 2 telephone numbers.
Effective Date
4) The principal must check the relevant box to denote whether they require 1 or 2 physicians to confirm that the principal is no longer able to make a health care decision.
Agent`s Powers
5A) The principal must signify whether or not they will require artificial nutrition and hydration.
- Initial to allow withdrawal or withholding of artificial hydration and nutrition.
- Initial to forbid withdrawal or withholding of artificial hydration and nutrition.
5G) The principal can describe other health care powers they wish to give their agent by initialing the relevant boxes.
- Determine what happens to the principal`s body after death.
- Give authority for an autopsy or postmortem after death.
- Delegate a new agent.
Authorization Of Anatomical Gifts
5H) The principal must describe any wishes they have regarding donation of an anatomical gift by first initialing and then checking the relevant box(s).
- To authorize an anatomical donation.
- Transplantation.
- Therapy.
- Research
- Education
- All the above
- Any required organs/tissues.
- Specified organs/tissues not to be used.
- To prohibit an anatomical donation.
Health Care Directive: Part 2
Withdrawing Or Withholding Life Prolonging Treatment
2) The principal must initial the relevant box(s) to denote withholding or withdrawing of specific life prolonging treatments.
- Artificial hydration and nutrition.
- Surgery and invasive procedures.
- Antibiotics.
- Artificial respiration.
- Radiation therapy.
- Heart-lung resuscitation.
- Dialysis.
- Chemotherapy.
- Any other procedures.
- All possible life prolonging procedures even if improvement of condition is not possible.
Validity
4) The details of the relevant persons are required to validate the document.
- Date.
- Signature of principal.
- Print name of signature.
- Witnesses signatures.
- Witnesses names.
- Witnesses addresses.
- County.
- Date.
- Name of principal.
- Signature of notary.
- Print name of notary.
HIPAA Privacy Authorization Form
1) The principal must name the agent who they authorize to have access to their `protected health information` (PHI).
2) The principal must designate a period of authorization for release of PHI.
- Check box and enter specific date period.
- Check box to authorize for any time when the agent is in authority.
3) The principal must specify which types of PHI they wish to be released by checking the relevant box.
- Complete personal health records.
- Complete personal health records while checking the boxes for the following exceptions:- mental health records, communicable diseases, alcohol/drugs/any other.
4) The principal can name other persons for whom they give permission to share their PHI with.
- Name of person.
- Relationship of person to the principal.
6) The principal can select the length of time this HIPAA form is authorized for.
- Enter the date until which the form is valid.
9) The patient must enter their details to show they understand the HIPAA document.
- Principal`s signature.
- Date.